
Schroth Method for Scoliosis and Hyper-Kyphosis:
OPTIONAL TELE-HEALTH AVAILABLE
THE SCHROTH METHOD
The Schroth Method is a 3 – dimensional treatment approach for people with idiopathic scoliosis, adult onset scoliosis and hyper-kyphosis. The purpose of this treatment is to help the patient learn a “self correction” of the scoliosis curve pattern. This includes postural re-education and decompression of the curve concavities in order to reduce curve progression. The Schroth Method focuses on chest wall expansion with targeted breathing and neuromuscular stabilization in order to support the “corrected” posture. This method includes scoliosis specific exercises – exercises that focus on the concavities of the curves to reduce compression and ultimately help reduce scoliosis progression. Scoliosis specific exercises are different from typical fitness or rehabilitation exercises in that they provide a “corrective” force to targeted areas of the curves. Fitness exercises cannot create the same “corrective” forces, and must be modified for people with scoliosis to prevent increasing compression which will simply strengthen the curve pattern.

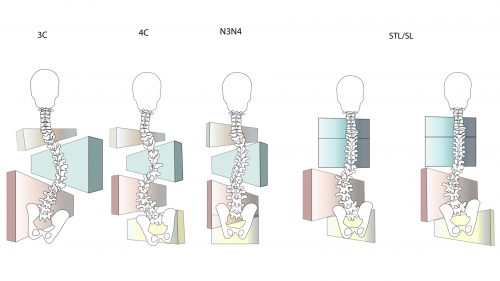
The Blocks are used to demonstrate the 3 dimensional nature of scoliosis. Block organization represents how scoliosis may affect the cervical, thoracic and lumbar spinal segments, and pelvis. Scoliosis specific exercises are uniquely designed for each individual based on the patient assessment and curve type.
 WHAT IS IDIOPATHIC SCOLIOSIS?
WHAT IS IDIOPATHIC SCOLIOSIS?
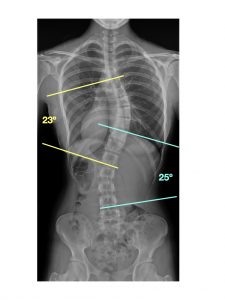
Scoliosis Research Society (SRS) defines Idiopathic Scoliosis (IS) radiographically. The SRS defines scoliosis as a lateral curvature of the spine greater than or equal to 10 degrees (Cobb angle) with rotation of unknown cause. Click here for more information. Structural changes of the vertebrae cause wedging and torsion. This leads to a 3 dimensional spine deformation. Many people do not understand the difference between a structural scoliosis and a functional spine asymmetry. A functional asymmetry is a muscle imbalance causing the appearance of spinal curves. The Cobb angle (curve angle) represents a structural scoliosis if it is at least 100. It is used by the SRS to inform treatment guidelines. A structural scoliosis must also demonstrate wedging and rotation that is greatest in the apical vertebra.
 Balanced 3-4 Curve Pattern
Balanced 3-4 Curve Pattern
General Treatment Guidelines: Adolescent Idiopathic Scoliosis
< 250 Cobb angle: Treatment Recommendation – Observation.
250-500 Cobb angle: Treatment Recommendation – Bracing
500 Cobb angle: Treatment Recommendation – Surgery
Age and bone maturity will affect these recommendations: see SOSORT Guidelines
Adult Scoliosis is divided into 3 categories:
1. Adult onset/De Novo = Primary degenerative scoliosis that starts later in life, mostly based on a disc and/or facet joint arthritis affecting those structures asymmetrically with predominantly back pain symptoms
2. Adolescent Idiopathic Scoliosis, stable or progressing into adulthood (may be combined with degeneration)
3. Secondary scoliosis (a) Due to: pelvis oblique, leg length discrepancy or hip pathology or as a secondary curve in idiopathic, neuromuscular and congenital scoliosis, or asymmetrical anomalies at the lumbosacral junction (b) In the context of a metabolic bone disease (mostly osteoporosis) combined with asymmetric arthritic disease and/or vertebral fractures.
Pain and Adult scoliosis: While some adults with scoliosis have pain and disability, research indicates that there is no correlation between the extent of the Cobb angle and pain (Schwab FJ et al Spine 2006). In fact, adult scoliosis is often more of a sagittal plane problem: flattening of the lumbar lordosis (sagittal plane curve) and increased posterior pelvic tilt. This is often the result of compensations for pain or degeneration (Schwab F at el. Neurosurgery 2013).
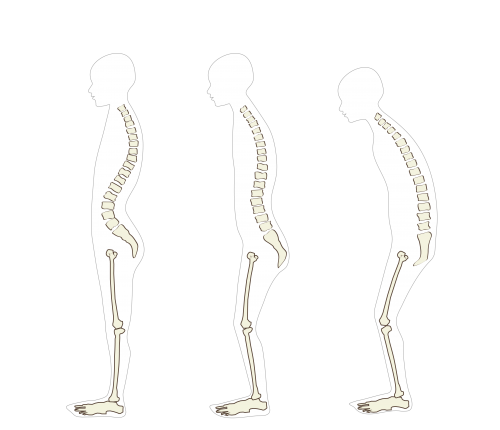
WHAT IS HYPER-KYPHOSIS AND SCHEUERMANN’S KYPHOSIS?
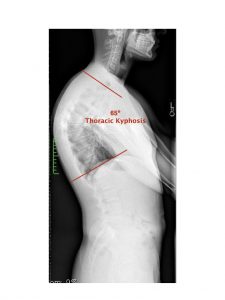
The normal kyphotic angle of the thoracic spine (upper back) is between 26 and 46 degrees (Bernhardt and Bridwell Spine 1989). Hyperskyphosis is therefor a flexion angle greater than 46 degrees. This produces the appearance of a “hunched” or rounded upper back. This postural dysfunction can affect the cervical and lumbar lordosis in the neck and low back causing pain. This postural dysfunction is often changeable. Scheuermann’s Kyphosis, however, is hyper-kyphosis that is a structural spine deformity. It is defined radiologically as a kyphotic angle greater than 40 degrees with anterior vertebral wedging greater than 5 degrees of 3 or more vertebrae (Sørensen KH. Copenhagen: Munksgaard; 1964). Click here for more information.


